Dsm 5 - Tumblr Posts
can’t a straight guy read a little gay literature?
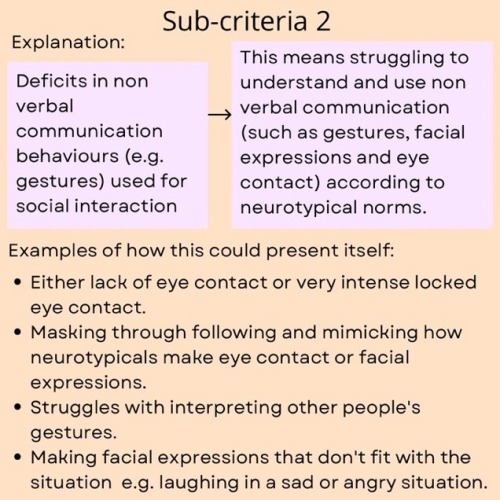
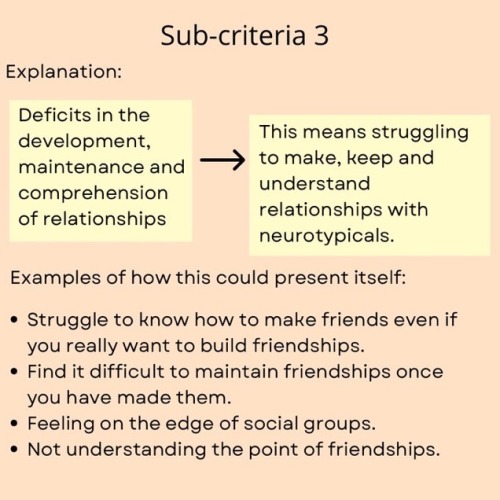
Autism Diagnosis Criteria Explained
@neuro_lou
it’s always “you need to get a job” and “why aren’t you in college?” And never “Ava what are the 5 DSM-5 criteria for autism, why don’t you tell me all about your opinions and theories on it?”
hardware vs software: mental disorder edition
I was trying to explain the difference between AuDHD and OSDD's source to an acquaintance the other week, found the note I wrote in my google keep, and thought it might be worth sharing.
I hope I have come up with a good way of explaining. I'm open to kind criticism.
Hardware: Neurodevelopmental disorders
Hardware cannot be changed. The brain is wired like that. Hardware includes ASD, ADHD, dyslexia, dyscalculia, dyspraxia, intellectual disability, some kinds of visual and hearing imparements.
It's like when you buy a laptop, it comes with a set of keys, screen, RAM etc, you can't really change it (you can if you force it but for now, think that you can't. Be like Apple, you get what you get!). Everyone has hardware, but it'll look different. Think, an autistic keyboard has a different set of keys to a neurotypical keyboard.
Software: things that develop out of trauma or stress
Software can be changed beyond the original purchase of hardware. It can be installed and added. However, unlike software, most disorders can't be uninstalled (but they can be improved with time and therapy).
Disassociative disorders (DID, OSDD, DPDR etc) install to manage trauma. Depression, PTSD and anxiety is software.. or even a bug... or... virus? is it a virus???
Some software is more likely to install on specific hardware types.
I also had a thought that communicating between neurodivergent people and neurotypicals as like trying to communicate apple with android, it doesn't always work perfectly, though often gets the point across, however sometimes it completely misses the mark??
Not an OSDD system, but as you (OP) said, a lot of it comes from back when OSDD was called DDNOS in the DSM IV.
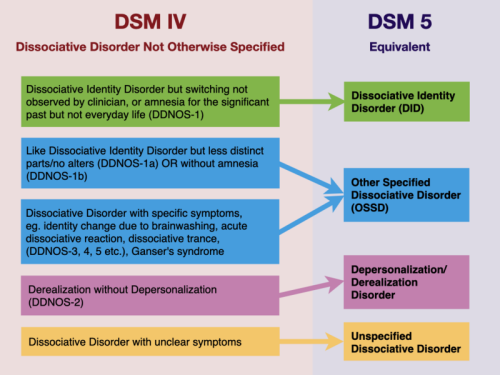
DDNOS-1a and DDNOS-1b were legitimate psych diagnoses pre DSM-V, and a lot of information was updated to say OSDD, but didn't take into account the removal of 1, 1a, and 1b (I wouldn't be surprised if people used find and replace on website resources)
DDNOS 1 – DID but switching not observed by clinician, or amnesia for the significant past but not everyday life. DDNOS 1a – Like DID, but with less distinct parts/no alters. Alters may be emotional fragments or the same individual at different ages. Can experience emotional amnesia rather than physical amnesia. DDNOS 1b – Like DID, but no amnesia between alters.
Similar to how some chose to continue calling themselves MPD, those that were diagnosed using the DSM-IV or earlier just chose to continue using those clarifiers, or they find adding the clarifiers create a shortcut to explaining their symptom set; especially in system spaces.
P-DID isn't recognised in the DSM, however it is used in the ICD* *Chapter 6 of the ICD specifically covers mental, behavioural and neurodevelopmental disorders. Moreover, while the DSM is the most popular diagnostic system for mental disorders in the US, the ICD is used more widely in Europe and other parts of the world, giving it a far larger reach than the DSM. An international survey of psychiatrists in sixty-six countries compared the use of the ICD-10 and DSM-IV. It found the former was more often used for clinical diagnosis while the latter was more valued for research.[14] This may be because the DSM tends to put more emphasis on clear diagnostic criteria, while the ICD tends to put more emphasis on clinician judgement and avoiding diagnostic criteria unless they are independently validated. That is, the ICD descriptions of psychiatric disorders tend to be more qualitative information, such as general descriptions of what various disorders tend to look like. The DSM focuses more on quantitative and operationalized criteria; e.g., to be diagnosed with X disorder, one must fulfill 5 of 9 criteria for at least 6 months - wikipedia (DSM). Who does your diagnosis and what country you are in will influence whether you're able to get a P-DID diagnosis; the same goes for complex PSTD. C-PSTD (complex ptsd) is only recognised as a diagnosis by the ICD, however there is hope that with the DSM-VI (DSM-6) that they may add C-PTSD as a differing diagnosis from PTSD.
Question for OSDD-1a/1b systems: Why do you use 1a/1b?
I ask because 1a and 1b do not exist within OSDD. What you're thinking of is DDNOS-1a/1b which are outdated. Similar to how MPD is the outdated term for DID. To my knowledge, OSDD-1a/1b has never been a thing before. OSDD is just OSDD or P-DID, depending on where you live. So where did this idea come from in system communities? You can't be diagnosed with OSDD-1a/1b, so if you've done extensive research to self diagnose with this, where did you get the idea that OSDD-1a/1b is a thing instead of just OSDD or P-DID? *DISCLAIMER: This is not asked out of hate. I am genuinely curious. Genuine answers will not be met with arguments.*
i put the DSM in BDSM
(i am severely mentally ill)
On Duke Thomas and the problem with the ASPD diagnosis
There are many many messed up things with the way personality disorders are classified in the dsm-5, but I think what best illustrates how fucked up the ASPD diagnostic criteria are is that Duke Thomas (yes, Duke Thomas, the Signal) could definitely get diagnosed with ASPD.
FYI, ASPD means Antisocial Personality Disorder, this is the clinical entity usually referenced when we talk about psychopathy or sociopathy. So how does that fit Duke? (It doesn't. And yet...)
First is the question of why should we diagnose Duke, a teenager whose personality is still in construction, with a personality disorder? Well, while you only get diagnosed at 18 (criteria B), your "transgressions" occur since age 15, which means Duke's behaviour in We are Robin (when he was a traumatized homeless teenager in a hellscape of a city)can 100% be used to spring a diagnosis on him at 18. Criteria D is just excluding schizophrenia and bipolar episodes. Now let's take a look at criteria A: at least three manifestations from this list of signs that someone is "disregarding and transgressing other people's rights" :
1. Repeated liable to arrest behaviours
So, like when Duke got arrested for being part of We Are Robin, then escaped arrest and did it again and again?
2. tendency to lie for either profit or pleasure: repeated lies, use of pseudonyms or scamming.
Funnily enough, I don't think Duke had a pseudo in WAR aside from Robin ofc (feel free to correct me if I misremember) but Isabella and the others sure did! Still, when Duke gets arrested, he lies and insists he isn't part of the WAR and hasn't done anything illegal, which fits the criteria as "lying for personal profit". (If you're feeling full of righteous rage reading this it's normal, I'm trying to prove a point.)
3. Impulsivity OR inability to plan ahead.
Duke is definitely able to plan ahead, but I know very few clinicians who, upon hearing how this mf jumped off a bridge to escape a moving police car, wouldn't write down "impulsivity"... And it's not like it's his only similar offence. I'm not saying he is impulsive, but that behaviour is definitely enough to get him classified as one in the eye of a clinician, especially if they're meeting him after an arrest and hearing from that episode second-handedly.
4. Repeated fights and aggressions.
Do I need to develop why this would fit Duke?
5. Inconsiderate disregard for his safety OR other people's safety
If you thought I was being unfair about the impulsivity for jumping from a bridge, you can't tell me this doesn't fit here. Again, far from the sole iteration of it from Duke in WAR, but one of the most memorable.
6. Persistent irresponsibility: this one is all about pathologizing and shaming financial and employment struggles, which is its own nest of issues but doesn't concern our boy Duke since he isn't an adult.
7. justification/indifference after harming, stealing or mistreating someone (lack of remorse).
The question here is, does street vigilant violence count as harming someone? I'm gonna go with yes, because there is no question of whether it is justified, and attempting to defend oneself is here considered a sign of a lack of remorse. (Whether or not you count it doesn't matter so much though, because we're already over three hard yesses.)
So, to recap, whether or not we count criteria 7 and 3, Duke already fits the bill of 3 criteria, and thus fits criteria A.
The last criteria to examine, criteria C, is :
"manifestations of a conduct disorder before 15". So you're going backwards in time investigating the person's past actions to see if they fit the criteria having, most of the time, only data like police records, grade reports, foster care interviews sometimes, on top of your own retroactive bias. To quote Duke's bio "during his time in foster care, Duke went from an upstanding student to becoming a bit of a delinquent, receiving poor grades and racking up an extensive police record due to his investigations into his parents." I'm not gonna go through the whole list of conduct disorder symptoms because there is so many, just know the cutoff is 3. For Duke, we can identify: "picks up fights", "stays up late at night despite interdiction from his guardians (before 13 -when was Duke first placed?), "often skips school" (again, before 13), "has run away and spent the night outside at least twice or once but didn't come home for a long time", "has b&e into someone's house/car/building" (i'm pretty sure that happened at some point? An abandoned building that legally belongs to someone else counts btw), "lies often to avoid obligations". I might have missed some from Duke's time in foster care so feel free to point out any sign of conduct disorder I didn't spot!!
In conclusion, Duke fits the criteria for ASPD and would have been, in universe, liable to be diagnosed as soon as he turned 18 (which could very well had happened if he had stayed in the system or gotten arrested). So, is the conclusion that Duke Thomas actually has ASPD? Obviously not. The point is the dsm criteria for ASPD (and conduct disorder) are so fucked up that fictional superheroes who definitely don't have it meets them on a technicality. Even if we accept ASPD as a valid clinical entity (which is highly debatable) this wording is so wrong I can't wrap my head around this.
Another point you might have noticed is that post-crisis Jason Todd (Jaybin, not the Red Hood) would also have been a very valid test to highlight how problematic these criteria are. While little Jason is at risk because there is also a huge classism problem in these criteria (which don't do shit to acknowledge necessity theft and actively shame financial insecurity), Duke is at risk because studies have highlighted the racist bias in these criteria: regardless of clinical intent, the awful, unclear wording of these criteria have led to a huge race difference in ASPD diagnosis. Add to that the foster care to prison pipeline, a story where Duke had been diagnosed with ASPD would have been all too realistic (assuming dc writers know about aspd).
All these critiques are acknowledged in the DSM-5: Revised Text version, where researchers warn against the bias and unclear wording of these criteria. But let's be honest: clinicians barely ever read the diagnostic characteristics of the original DSM-5, let alone the revised text (generally because 1. They're overworked and 2. To interview properly, you need to ask questions based on the criteria while talking to the person, which is super hard and means you need clear, defined, easy to memorize criteria). So most of the time, clinicians just base themselves on the diagnostic criteria. Just saying "hey careful about bias these criterias aren't that well written" in the revised text isn't enough : if ASPD is going to stay an entity at all, it needs better criteria.
The ASPD criteria are amongst the worst failures of the DSM-5, and the case of Duke Thomas perfectly illustrates the pitfall in which we might fall if we don't remain critical of classifications and take into account how they fit within a social and political sytem.
*This post simplifies listed criteria to what clinicians actually use while diagnosing for clarity's sake, but doubting your sources is smart, so feel free to check out the detailed criteria to check I'm not misinterpreting what the dsm says by simplifying it since the DSM-5 is available online for free, search key for ASPD is F60.2 and for conduct disorder is F63.81.
Fun hang out idea!
We go to our local library and I read the DSM 5 while you play on your phone and I occasionally tell you fun facts. :3